The Progressive Goal Attainment Program (PGAP®) is an evidence-based treatment program targeting psychosocial barriers to recovery and rehabilitation for clients suffering from debilitating health or mental health conditions. It is a highly researched standardized intervention for reducing disability associated with a wide range of debilitating health and mental health conditions. The PGAP is supported by empirical data and has been demonstrated to reduce disability and contribute to successful return-to-work in individuals with conditions including back pain, whiplash, fibromyalgia, cancer, depression, and PTSD.
The primary goal of the PGAP is to reduce psychosocial barriers to rehabilitation progress. This goal is achieved through the use of evidence-based techniques specifically designed to target psychosocial risk factors.
The PGAP includes:
• Cognitive-behavioural techniques such as thought-monitoring and reappraisal;
• Behavioural techniques such as graded exposure and goal setting;
• Relational techniques such as disclosure and validation.
The PGAP would be considered a CBT intervention, with a primary focus on behaviour change. CBT techniques have been adapted such that ‘disability reduction’ is the central objective of treatment as opposed to symptom management.
Finally, the evidence base speaks clearly in favour of the PGAP, particularly as it pertains to return-to-work outcomes. In all clinical trials of the PGAP, return to work has been the primary outcome variable. A list of scientific publications supporting the use of the PGAP as a return-to-work intervention can be accessed through the www.PGAPworks.com website.
Within our team, both Kelly Alderson and Cass Hill are trained and experienced in the provision of the Progressive Goal Attainment Program. We have found it to be of extreme benefit to the majority of clients who have engaged in the program. For more information on how the PGAP can assist you or your clients or to find out more information regarding this service, please feel free to contact us for further discussion.

The general health benefits of daily walking have been widely documented and include healthy weight maintenance, improved heart health, improved sleep patterns, reduced stress and boosting mood. These benefits are even more pronounced when recovering from a workplace injury.
One of the biggest barriers workers often face after an injury is a loss of physical fitness and a general decrease in activity levels. Many injured workers report withdrawing from a variety of activities they previously enjoyed, leading to a variety of health issues in addition to their original injury.
Walking is an activity that is widely accessible to most people who have suffered an injury and can be easily adjusted to compensate for a variety of restrictions.

Exposure to sunshine adds the extra benefit of boosting Vitamin D levels which have found to be deficient in around 30% of Australians. Vitamin D supports bone health by regulating calcium levels in the blood and maintaining a healthy skeleton.
Walking also positively effects mental health with benefits including clearing the mind, increasing general energy levels, reducing symptoms of depression and boosting self-esteem.
Embarking on a 30 minute walk every day has even been related to an increase in natural pain killing endorphins.
So what are you waiting for? Start a walking program today!


Article Review by Kelly Alderson
The Vocational Rehabilitation Index (VRI) is a tool which can measure personal factors in return to work after a compensable injury. In this research, data was collected from 461 participants in NSW who had a Whole Person Impairment over 10%.
The VRI considers
| Personal | Most Risk | Lower Risk |
| Age^ | 41 – 50 years old | 31 – 40 (16 – 30 close to this) |
| Gender^ | Male | Female |
| Occupation | Unskilled (low skilled roles) | Professionals |
| Length of time away from work^ | Over 2 years | 13 – 24 months |
| Spinal Injury*1 | Disc injury (lower back) | Whiplash |
| Psychological Condition*2 | Minor and Major conditions | No psychological condition |
| Labour Market* 3 |
*1 Spinal Injuries – there was no evidence that the seriousness of spinal injury is a predictor.
*2 Psychological conditions – these were broken into major and minor. Across both of these domains, the people presenting with these conditions were approximately 3 times less likely to return to work. What is not clear in this article is if there is any difference between those with a primary or secondary claim and the absence or presence of a psychological condition that is not compensable. However, I think we could draw some inferences about this. Interestingly, this did not meet the threshold for statistical significance. It may be that if these items were teased out further, that there may be an effect that would meet the requirements for statistical significance.
*3 Labour Market – We contacted the author about this and he did clarify this point. He advised that less than ¼ of participants had returned to work. He further explained that the data was drawn from areas of high unemployment and so the labour market did not seem to have an effect, but he did note that this created some bias in the data.
^ denotes that the finding met the threshold for statistical significance.
The above table provides a profile for risk which can be helpful for determining whom might be suitable to refer for vocational rehabilitation services, although there are probably other triggers that should be considered also. For example; perceived injustice, poor relationship with the pre-injury employer and failure to engage with a return to work plan.
In regards to time away from work, it is interesting that this research suggests that the best return to work rates came out of the 13 – 24-month cohort. Although, it is important to note that this data is related to those with a whole person impairment over 10%. In regard to risk, those with an injury around the 12 month mark were also at higher risk and therefore need careful consideration.
We asked the author a couple of questions about the research, in particular if they thought that there is a link between occupation (unskilled or low skill) and readily transferable skills. Dr Athanasou agreed with this observation and added that this is also reflective of the data set and it being drawn from areas with higher levels socioeconomic and sociocultural disadvantage. So it is possible that other confounding variables may be at play as well, in terms of what we know about socioeconomic disadvantage. For example, poorer health outcomes (ABS, 2018a) because people in this group tend to access less preventative health services, they are at high risk of social exclusion, have more difficulty affording noncompulsory education, in fact year 12 completion rates have increased nationally, but there is no evidence that those residing in high levels of socioeconomic disadvantaged have followed this trend (ABS, 2018a). It is a hypothesis of mine, that part of the picture in terms of return to work, is that a work injury is likely to have a larger impact on this group because of pre-existing disadvantages and this is likely to deepen should redeployment be required. This adds an additional layer of complexity to an already complex picture.
With this in mind, we then need to look forward to solutions. Truth be told, there are a bunch of solutions that are well outside of the scope of Return to Work, for example improving base level language and literacy skills. Although this is important, it is not always going to be achievable, but there are some other considerations. For example, in terms of suitable duties plans, are we wasting a potential opportunity here? Don’t get me wrong, I am not suggesting that we ‘throw the baby out with the bath water’ and stop them as they are critical for other reasons. But there is more need now than ever before to make sure that these are targeted and timely because wasting 6 months in a work placement that is not going to lead to employment and is not serving the worker any skill development opportunities, is potentially wasting valuable time. Sure, if you are 100% confident that the person will get back to pre injury duties, it is probably fine. However, if you are sitting on the fence in terms of a goal, then based on this article, the best bang for your buck in terms of a placement is developing potential employability skills that are currently missing or underdeveloped (this may require some vocational counselling to workout an alternative goal and what needs to be achieved skill wise). This way, best case scenario the person returns to work and they have learnt some new skills, but worse case scenario, the goal needs to be reviewed and the person has already tried out another role and has already started accumulating the skills required to be successful in securing employment (plus they have a reference who will be able to hopefully help them secure that next job (if it does not arise out the placement).
So the next issue is how can we get employers to engage in mentorships for their staff or those needing a placement. But I think that this is a topic for another day.
If there are other topics you would like us to review or review, please comment below and we will add this to our list.
Reference:
ABS . (2018a, March). http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4250.0.55.001Main Features32009.
ABS. (2018b, March). http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by Subject/1370.0~2010~Chapter~Socioeconomic disadvantage (4.1.7.4).
Athanasou, J. (2018). A Vocational Rehabilitation Index and Return to Work after Return to Work after Compensable Occupational Injuries in Australia. The Australian Journal of Rehabilitation Counselling, 69-78.

While engaging in a reskilling work placement with Civil Train SA at the Chinese Association at Findon, some of our Return to Work participants made an amazing discovery!
On removing some temporary boards in the front foyer of the building, they uncovered original artwork done by famous Indigenous artist, Les Huddleston in 1975 when he was just 16 years old.
Since then they have been undertaking research and attempting to contact the artist and local art galleries to find out the best way to display this newly discovered artwork.
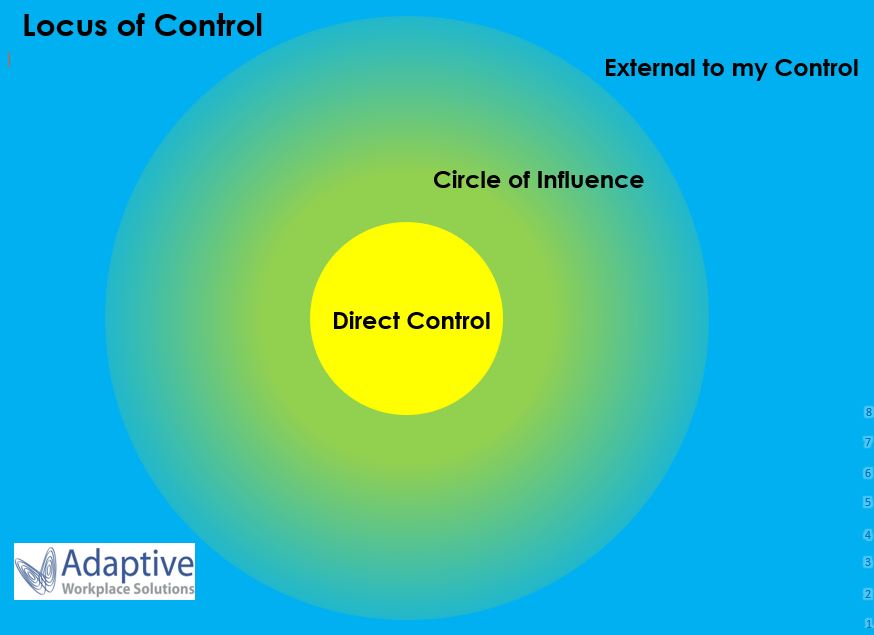
Locus of Control is the extent to which people believe they have power over their lives. This concept was developed by Julian Rotter in the 1950s and is widely accepted within psychology today. We have observed that many of our clients who have difficulties with successfully returning to work after an injury have an external locus of control, in other words they believe that outside forces are directing their personal outcomes. They often focus excessively on worries or concerns that are external to their control and don’t tend to take responsibility for their own successes or failures. Most of their energy is spent in the blue section of the image above. This can serve as a barrier to their progress and return to work goals. As a comparison, people who have an internal locus of control believe that they can influence events and take responsibility for their own actions and outcomes. They invest their energy in the yellow section of the image above, focusing on what they can either directly control or have some level of influence over.
If you are noticing a worker who blames others for their lack of progress, puts events down to fate or luck, expresses that other people (e.g. their doctor, employer) are in control of their situation or doesn’t take responsibility for their own actions (positive or negative) it might be that they need some assistance before they are able to move forward. Heightening their awareness of the parts of their life that they can influence is a key aspect of assisting with this. Opening up a conversation about what aspects of their current situation they feel are realistically outside of their control and then discussing the things that they can affect or impact is a great starting point. Positive goal setting can also be helpful as it draws attention to direct action they can take. If you have tried those steps and are finding your client is stuck in unhelpful thinking patterns, it may be that we can help! Adaptive Workplace Solutions have developed a tool shown in the image above which we have used with many clients with great results. When used along with counselling and home activities, we have had an excellent success rate of assisting clients to shift their locus of control, enabling them to gain a healthy level of control over their lives. Many clients have named it as pivotal in changing their perspective and allowing them to take steps towards returning to work.

Did you know that in addition to our permanent offices in South Plympton and Munno Para, Adaptive Workplace Solutions can provide services across all areas of Adelaide!
We frequently make use of an office space in Mount Barker and can also meet clients in libraries or quiet cafes if travelling to our offices is difficult.
We can also provide services in regional areas of South Australia via phone or video calls. Location is no barrier to accessing our quality personalised services.

At Adaptive Workplace Solutions we take a pro-active approach to injury prevention within our team. We consider workplace health and safety a priority and one of the latest additions to our offices are our sit to stand workstations.
The helpful staff at The Ergo Centre assisted us with deciding which product to choose for our needs and had our new workstations delivered and set up for us! Having the option of sitting and standing throughout the work day has been found to lead to better overall posture, more general activity and can also assist with lower back discomfort. Kelly and Cass are enjoying their new workstations and finding them of great benefit, standing more frequently throughout their work days.

Contact Us
(08) 8293 6783
admin@adaptivews.com.au